What is BPPV?
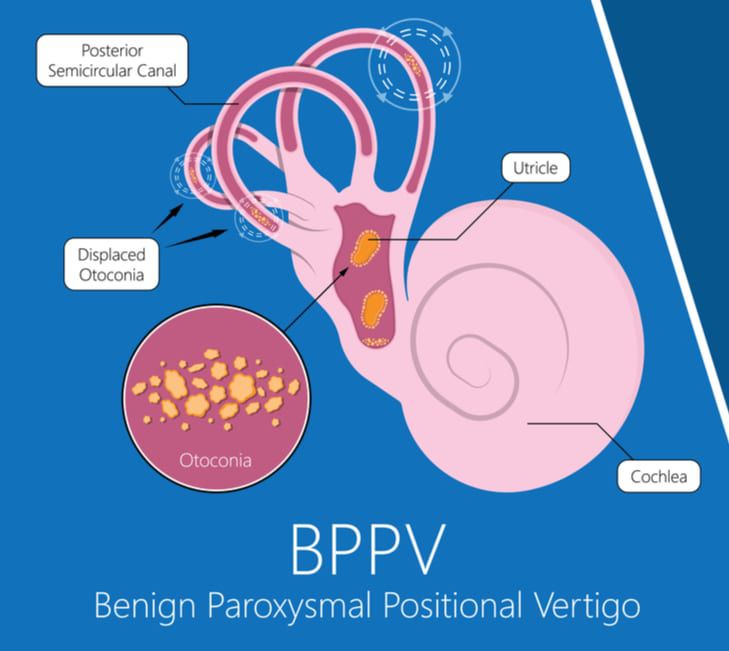
Benign paroxysmal positional vertigo also known as BPPV is a common cause of vertigo which usually gives the brief sensation of spinning or dizziness associated with moving the head.
BPPV is a mechanical problem in the inner ear. It occurs when some of the calcium carbonate crystals called “otoconia” that are normally embedded in a gel like substance in the utricle become dislodged and move into one or more of the 3 fluid filled semi-circular canals, where they are not supposed to be. When enough of these accumulate in one of the canals they interfere with the normal fluid movement that these canals use to sense head motion, causing stimulation of the nerves that detect head movement sending abnormal stimulation to the vestibular system causing dizziness, spinning, nausea and nystagmus (fast eye movements) .
Are there different types of BPPV?
There are two types of BPPV, one is where the loose crystals (otoconia) can move freely into the fluid of the canal this is called “canalithiasis”. The second type and more rarely experienced type of BPPV is where the crystals are thought to be ‘hung up’ or adhering on the bundle of nerves that sense the fluid movement, this is called “cupulolithiasis”. With the first type of BPPV “canalithiasis”, it takes less than a minute for the crystals to stop moving after a particular change in head position has triggered a spin. Once the crystals stop moving, the fluid movement settles and the nystagmus (fast eye movement) and vertigo symptoms will stop. With the second type of BPPV “cupulolithiasis”, the crystals (otoconia) become adhered on the bundle of sensory nerves which makes the symptoms last longer.
How is BPPV diagnosed & treated?
BPPV is diagnosed through a subjective and objective examination by a trained practitioner which involves tests like the Dix-Hallpike, side lying test & roll test.

The right Dix-Hallpike position used to elicit nystagmus and vertigo symptoms for diagnosis. The patient is moved from a seated position to laying on their back with their head turned 45 degrees to the right and held for 30 seconds with the eyes open and physiotherapist watching all eye movement.
The nystagmus (fast eye movement) will have different characteristics that allow a trained practitioner to identify which ear the displaced crystals are in, and which of the 3 canal(s) they have moved into. Tests like the Dix-Hallpike or Roll Tests involve moving the head into specific orientations, which allow gravity to move the dislodged crystals and trigger the vertigo while the practitioner watches for the movements and determines the direction and timing of the nystagmus (eye movement).
Once your physiotherapist has diagnosed which canal(s) the crystals are in, and whether it is canalithiasis or cupulolithiasis, then they can take you through the appropriate treatment maneuver for you.
The maneuvers make use of gravity to guide the crystals back to the chamber where they are supposed to be via a very specific series of head movements.
Studies and research have shown that precision of the maneuver is the key to successful treatment and therefore it is recommended that this are completed by a trained professional.
Additionally, there is a screening tool completed by your trained practitioner prior to performing testing such as neurological examination and neck screening, along with other safety-related investigations to determine if certain elements of the procedure need to be modified or avoided.
How long does it take to treat?
Studies have shown that effectiveness of BPPV treatment is well into 90% improvement by 1-3 treatments by a trained professional. The “Cuplulolithiasis” “hung up” type can take a few more sessions as can BPPV as a result of trauma/head injuries. Once the crystals (otoconia) are back in the correct place and the symptoms have stopped, people can often feel some mild residual sensitivity to motion and unsteadiness. If is important that you follow up with your vestibular therapist so that they can evaluate this and provide home exercise techniques that can assist with correcting this.
Which symptoms BPPV doesn’t cause?
Please be aware BPPV will not give you constant dizziness that is not able to be changed or reproduced by a movement or change of position. It does not cause hearing loss, fainting, headaches or neurological symptoms. IF you have any of these symptoms, you must tell your health care provider immediately as other vestibular disorders can be misdiagnosed as BPPV.